The drug has been developed by DRDO’s Institute of Nuclear Medicine and Allied Sciences (INMAS) in collaboration with Dr Reddy’s Laboratories
New Delhi, May 17
Defence Minister Rajnath Singh and Union Health Minister Dr Harsh Vardhan on Monday released the first batch of Anti-COVID drug 2-deoxy-D-glucose (2-DG) developed by the Defence Research and Development Organisation (DRDO).
The drug has been developed by DRDO’s Institute of Nuclear Medicine and Allied Sciences (INMAS) in collaboration with Dr Reddy’s Laboratories. DRDO Chairman Dr G Satheesh Reddy said that DRDO and Dr Reddy’s lab had gone through the complete trials and conducted trials across 30 hospitals and on a large number of patients. The first batch of 10,000 doses of 2DG medicine would be launched early next week, informed DRDO officials told ANI on Friday.
The drug comes in powder form in a sachet, which is taken orally by dissolving it in water. It accumulates in the virus-infected cells and prevents virus growth by stopping viral synthesis and energy production. Its selective accumulation in virally infected cells makes this drug unique.
In the ongoing second COVID-19 wave, a large number of patients are facing severe oxygen dependency and need hospitalisation. The drug is expected to save precious lives due to the mechanism of operation of the drug in infected cells. This also reduces the hospital stay of COVID-19 patients. ANI
Barge with 273 on board adrift near oil rigs, Navy sends rescue team
Another one with 137 on board adrift some 15 km west of Mumbai
Tribune News Service New Delhi, May 17
A massive rescue operation has been launched at Arabian Sea after a ‘barge’ – an engineering ship — working near the off-shore oil-rigs of ‘Bombay High’ is adrift – meaning powerless to control itself.
There are 273 personnel on board. A free-floating barge in the ongoing cyclonic winds can be of a risk to other ships and also to the oil installations which are some 70 km south-west of Mumbai.
Indian Navy spokesperson in New Delhi Commander Vivek Madhwal confirmed that a request for assistance has come from Barge ‘P305’ adrift off Heera Oil Fields in Bombay High area. “It has 273 personnel on board, INS Kochi has sailed out from Mumbai with despatch for search and rescue (SAR) assistance. INS Talwar is also preparing to sail out,” Commander Madhwal added.
Meanwhile, the Navy has got another SOS call. A Barge ‘GAL Constructor’ with 137 people onboard is adrift some 15 km west of Mumbai. INS Kolkata sailed out on Monday afternoon to render assistance.
Both the barges may have to be tugged back into port if engines have failed or the water had filled in the engine room – normally at the lowest deck of the ship.
Several other ships and aircraft have also been readied for tasking in the wake of Cyclone Tauktae, he added.
Miniscule bleeding, clotting events post Covid-19 vaccination in India: Govt
Over 13.4 crore doses of Covishield vaccine have been administered as on 27 April in Indi
A beneficiary receives a dose of Covid-19 vaccine at a vaccination centre in Kullu. PTI
New Delhi, May 17
India has reported 26 potential cases of bleeding and clotting after administration of Covishield vaccine, a government panel investigating adverse events following Covid-19 immunisation has found.
The Union Health Ministry said in a statement on Monday that over 23,000 adverse events have been reported since the vaccination drive involving Covishield and Covaxin vaccines started in the country and of these 700 cases were reported to be serious.
The National Adverse Event Following Immunisation committee (AEFI) has completed an in-depth case review of 498 serious and severe events, of which 26 cases have been reported to be potential thromboembolic (formation of a clot in a blood vessel that might also break loose and carried by the blood stream to plug another vessel) events – following administration of Covishield vaccine – “with a reporting rate of 0.61 cases/ million doses”.
“There were no potential thromboembolic events reported following administration of Covaxin vaccine,” the ministry said.
As alerts were raised in some countries on post-vaccination “embolic and thrombotic events” on March 11 particularly with AstraZeneca-Oxford vaccine (Covishield), a decision was taken to conduct an urgent in-depth analysis of the adverse events (AE) in India in the light of global concerns, the ministry said.
The National AEFI committee noted that as of April 3, 7,54,35,381 vaccine doses had been administered (Covishield – 6,86,50,819; Covaxin – 67,84,562).
“Of these, 65,944,106 were first doses and 9,491,275 second dose. Since the Covid-19 vaccination drive was initiated – more than 23,000 adverse events were reported through the CO-WIN platform from 684 of the 753 districts of the country.
“Of these, only 700 cases (@ 9.3 cases /million doses administered) were reported to be serious and severe in nature,” the statement said.
“The AEFI data in India showed that there is a very miniscule but definitive risk of thromboembolic events. The reporting rate of these events in India is around 0.61/million doses, which is much lower than the 4 cases/million reported by UK’s regulator Medical and Health Regulatory Authority (MHRA). Germany has reported 10 events per million doses,” the statement stated.
Thromboembolic events keep occurring in general population as background and scientific literature suggests that this risk is almost 70 per cent less in persons of South and South East Asian descent in comparison to those from European descent.
The ministry is separately issuing advisories to healthcare workers and vaccine beneficiaries to encourage people to be aware of suspected thromboembolic symptoms occurring within 20 days after receiving any Covid-19 vaccine (particularly Covishield) and report preferably to the health facility where vaccine was administered.
The symptoms listed are breathlessness, pain in chest, pain in limbs/pain on pressing limbs or swelling in limbs (arm or calf), multiple, pinhead size red spots or bruising of skin in an area beyond the injection site, persistent abdominal pain with or without vomiting, seizures in the absence of previous history of seizures with or without vomiting, severe and persistent headache with or without vomiting (in the absence of previous history of migraine or chronic headache).
The symptoms also include weakness or paralysis of limbs or any particular side or part of the body (including face), persistent vomiting without any obvious reason, blurred vision or pain in eyes or having double vision, change in mental status or having confusion or depressed level of consciousness or any other symptom or health condition which is of concern to the recipient or the family.
The ministry said that Covishield continues to have a definite positive benefit risk profile with tremendous potential to prevent infections and reduce deaths due to Covid-19 across the world and in India.
Over 13.4 crore doses of Covishield vaccine have been administered as on 27 April in India.
The ministry is continuously monitoring the safety of all Covid-19 vaccines and is promoting reporting of suspected adverse events.
WHY INDIA SHOULD GIVE A LARGER ROLE TO MILITARY IN COMBATING COVID-19
India’s armed forces have 1.5 million trained personnel deployed across the country Last year, when the United States was battling with the surge of COVID-19 cases, its military docked two naval warships—USNS Mercy and USNS Comfort—on the coasts of New York and Los Angeles. Similarly, France had triggered ‘Operation Resilience’ to respond to the outbreak by involving large number of military personnel. The Great Britain also launched its biggest ever homeland military operations in peacetime to assist overwhelmed local hospitals treating patients. More controversially, in some parts of Europe, troops were deployed to enforce mandatory lock-downs by patrolling the streets, constructing roadblocks and curbing movement. Here, in India, from warplanes to warships, armed forces are being deployed to combat the catastrophic second wave of the pandemic. Besides bringing critical medical oxygen and other lifesaving equipment, Indian military has built multiple make-shift field hospitals. With record number of new COVID-19 patients, the country is facing shortage of medical facilities like hospital, medical oxygen and medical staff. It is indeed a war-like situation except this time enemy is not China or Pakistan but rather an invisible virus. And experts believe that there is only a minuscule percentage of their (military) capability has been put to use. Only the military health resources (Army medical corps) have been fully engaged and, there are other capacities available with military and those are not being fully utilised. Less than one-tenth capacity of the armed forces is being engaged. For example, during 2014 flood in Jammu and Kashmir, Indian Army not only provided relief and rescue to the general public, but also made the then chief minister of state, Omar Abdullah to speak to his officials by using military communication network. The communication infrastructure was totally down because all towers were flooded. Lt General D.S. Hooda, who was the northern army commander during J&K flood, has a fair idea of what a military can do in the time of health crisis. “While military health resources are fully committed to assist civil administration, there are other expertise and capacities available with the armed forces that are not being fully tapped. Army has experts from other fields like engineering, infrastructure and logistics,” Lt Gen Hooda told THE WEEK. During the massive earthquake in Jammu and Kashmir in 2005, Lt Gen Hooda also led the military rescue and relief efforts in the Uri sector. In the UK, its armed forces were working on 70 different tasks, from testing in schools to the rollout of vaccines and to support organisational and logistical efforts. China has reportedly mobilized over thousands of military personnel and set a world record of setting up hospitals in Wuhan, the epicentre of COVID-19 pandemic, in five days. India’s armed forces have 1.5 million trained personnel deployed all over the country and, by now, they all are COVID vaccinated. Some feel that the reluctance on part giving larger role to military could be a reflection on government’s inability to deal with the situation. But, General Deepak Kapoor, former Army Chief has a different take. He said that if the primary role of the military has been maintained and there is surplus capacity, then it should be roped in. While not in support of giving larger role to military, he said “You would not expect, especially when crisis in Eastern Ladakh has been fully resolved. And summer season is approaching, and there is a possibility of repeat of Chinese misadventure. We need to tackle the Chinese as well on the border.” In the past, the military has been on the forefront in relief and rescue operations during natural calamities like flood, cyclone and earthquake. Military experts claim that the fight against COVID-19 should be treated as a warlike situation. And every action has to be taken according to the Union War Book. The ‘War Book’ documents the role of each ministry at the time of war. Some believe that COVID is not only a medical emergency, as it is also a supply and logistic as well information emergency. And the military is equipped to create infrastructure in war footing. Military engineering services can be used to bring up the capacity of oxygen generation along with creating additional make-shift hospitals and dispensaries. Its strength of over 2000 officers can quickly set up the required infrastructure in short deadline in every place around the country. Even a cricket stadium can be converted into a make-shift hospital, if required. Meanwhile, combat engineers can be used for creation of structures like Corps of Signals units which will be handy for managing information like setting up emergency command and control room to track the movement of essentials in addition to the civil administration. On the medical side, the Army has an all-India network of medical store depots that can be used to supply of critical medicine to assist civil administration. “We deliver medicine to our forward most areas, even high altitude Siachen, with a strong supply chain. The Army Medical Corps does carriage of these medicines,” an official said. The official believes that with this, shortage of critical medicine can be handled to some extent. In addition, military has a huge logistic network with trained manpower. Army has a pan-India movement control network mechanism. And it can be used to track medical supplies. Movement Control Office (MCO) is responsible for assisting in planning, coordination and control of military movements in support of operations, exercises and administrative deployments across the country. “It can also be used in tracking critical medical supplies. It is a complete transparent method,” Lt Gen Hooda said while suggesting a unified command and control centre. Moreover, Army Service Corps has a large number of vehicles and transportation, which can be used for system and logistic support for a dedicated supply chain. Engineers from EME Corps can be utilised for repair and maintenance of heavy medical equipment. In Agra, the Army and the Air Force helped the district administration set up a new oxygen generation plant to meet the dire shortage of oxygen. Similarly, EME (electronics and mechanical engineers) personnel repaired an oxygen generation plant in Etawah district of Uttar Pradesh. In order to handle oxygen crisis, military officials believe that there could be a National Control Centre to streamline supply of oxygen. As per logistics principle, whenever there is scarcity of something, there should be a centralised control on it. “From oxygen plant to movement of container, every movement can be tracked through check post in the dedicated route,” the officer said. No one can forget incidents of Mumbai’s Elphinstone Road railway foot over bridge collapse and 2010 Commonwealth games bridge collapse, where Army came into the rescue and built those bridges in record time. With its pan-India presence, the Army can help civil administration provide the ground situation in remote areas with number of COVID-19 affected cases and available medical facilities. Following the UK model of testing and vaccination, the military can be roped in for the inaccessible remote areas. Thousands of British soldiers were supporting community testing. In India, with military’s presence in far-flung areas of northeast to hilly Ladakh, it will play a major role in supporting the civil administration. During multiple meeting with top military hierarchy, Defence Minister Rajnath Singh had conveyed that the armed forces need to pitch in a big way to assist the government in its fight against coronavirus, like the setting up of COVID facilities, transporting relief equipment and airlifting medical personnel within the country. While directing the armed forces to extend all possible assistance to the civil administration to tide over the crisis, Rajnath Singh also enhanced emergency financial powers to the forces. The armed forces have approximately 13,000 officers (doctors and nursing officers) and one lakh medical support staff. But, only 600 medical personnel from the armed forces, including doctors, nursing staff and paramedics have been deployed in various COVID facilities run by the defence ministry across the country. More personnel need to be deployed in such centres. It is learnt that since the military hospitals are packed with patients that include serving personnel and their dependents, it is difficult to spare more hands for civil duties. Veteran officers and medical personnel can nearly double the existing resources. While calling medical officers from the frontline formations for their deployment in various COVID-19 hospitals and medical facilities, the government has given extension to the short service commission doctors in the Armed Forces Medical Services, who are due for retirement. The Indian Air Force carried out 534 sorties from various parts of the country and 84 international sorties to transport cryogenic oxygen storage containers and other medical equipment. The medical equipment has been procured from Singapore, Dubai, Thailand, United Kingdom, Germany, Belgium, Australia, Indonesia and Israel. It’s not just the IAF, but the Indian Navy, too, is part of mission oxygen now. Nine Indian Navy warships have been deployed for the purpose and bring medical supplies. Close to 750 beds in various military hospitals have been set aside for civilian use. The AFMS (armed forces medical services) has also dedicated 19 hospitals, over 4,000 beds and 585 ICU units across the country. More COVID health care facilities and hospitals are being made regularly—a 150-bed hospital has been set up in the hostel of Punjab University by the Western Command. The DRDO has constructed four COVID hospitals in Delhi, Ahmedabad, Lucknow and Varanasi. Incidentally, except the one in Delhi, all three have been set up in the parliamentary constituencies of the prime minister, the Union home minister and the defence minister. Besides, defence scientists from DRDO’s Nuclear Medicine and Allied Sciences (INMAS) have developed an anti-COVID therapeutic application of the drug 2-deoxy-D-glucose (2-DG). Now, with the apprehension of third wave of COVID, requirement of medical facilities is going to multiple. And, using military along with civil administration can play a critical role in India’s fight against the pandemic. Major General Shashi Asthana (Retd), former Director, Operations and Logistics in the Army headquarters, says that the pandemic will have to be fought like war. He says the Army has a strong logistic network as they do the six months of winter stocking for entire northern command. From a pair of socks to ammunition, the Army logistics provides everything on time. “While the military is engaged in large numbers, there is also a scope to incorporate logistics expertise of the armed forces in crisis management to improve the supply chain,” Asthana said, adding that engineering resources of military can divert manufacturing assembly lines of other gases to oxygen to overcome the oxygen crisis. While recommending to keep the defence services in the decision making loop, Maj Gen Asthana was equally apprehensive about the government’s intention as currently the Indian military has no representation in any of the 11 empowered groups. Last week, Delhi Deputy CM Manish Sisodia had written to Union Defence Minister Rajnath Singh to lend services of the armed forces to the state to help it set up, operationalise and run COVID health facilities with about 10,000 oxygen and 1,000 ICU beds along with transportation of medical oxygen. The Ministry of Defence, however, turned down Sisodia’s request by saying they (military) are providing “as much help as possible” without compromising their operational readiness. Calling military for help is also a double-edged sword, politically. Had any elected leader called its help, it would led to criticism from his or her opponents that the administration has failed to perform. While suggesting that the Army should not take control of the situation, Lt Gen Hooda said, “It is not that the Army is a solution to every problem, but here you have a well-trained and disciplined military force. They can assist by carrying out testing and vaccination roll out to the areas with the Army’s pan-India presence including remote and border areas.”
ARMY STATEMENTS ON TRANSFER OF DELHI’S BASE HOSPITAL COMMANDANT FAIL TO STEM ‘VVIP’ ROW
The Indian Army for the second time in two days issued a statement on Thursday on the controversial transfer of Maj Gen Vasu Vardhan, the commandant of the force’s 1,000-bed Covid care facility in Delhi. Maj Gen Vardhan, one of India’s top pulmonologists, has been on the job for 18 months at the Army’s Base Hospital Delhi Cantonment (BHDC) and has served there with distinction. In a highly unusual and abrupt move, he was transferred to the Research and Referral (R&R) Hospital in the city as an additional officer on May 10. The posting, which effectively renders him without any work, has come just three months before the officer is due to retire, and amid reports that he has had to pay the price for saying no to VVIP requests for the antiviral Remdesivir. The army in a carefully worded statement says that Maj Gen Vardhan was posted out as part of an “HR Management Plan”. It says that Vardhan retires in three months. In the same time frame his deputy Brig Sandeep Tareja will also be moving out of the hospital as he has been promoted to the rank of major general. This will not be in “the best interest of the establishment that is treating Covid patients” says the statement, and so another officer, Maj Gen SK Singh, has been appointed as the commandant of the base hospital “so that there is adequate overlap and continuity in the top hierarchy of the hospital in these challenging times”. Maj Gen Singh is a plastic surgeon and was a deputy commandant of the AMC Centre and College in Lucknow. The army also says that Maj Gen Vardhan can use the three months at his disposal to destress and plan his future. The statement isn’t cutting much ice within the army. A senior officer says, “At a time when we are recalling doctors who have retired from the services to meet the crunch, do you really have the luxury to give a Covid doctor time to destress and send him on a punishment posting because he didn’t oblige the powers that be?” At the base hospital, there is dismay. Sources say Dr Vardhan, who lost his mother a few days ago, reported back on duty the same day. He has been “an inspiration” at a particularly challenging time when the hospital is overflowing with patients and is short of everything including doctors and nurses. At one time the hospital was even critically low on oxygen supplies. An SOS call that went public was not received well by authorities. But there have been complaints as well. A retired brigadier, infected with Covid, didn’t get a bed at the base hospital and died on his way to Mohali. A retired lieutenant general had written to the Chief of Defence Staff (CDS) Gen Bipin Rawat as well, complaining that veterans and their families were not being looked after well by the base hospital.
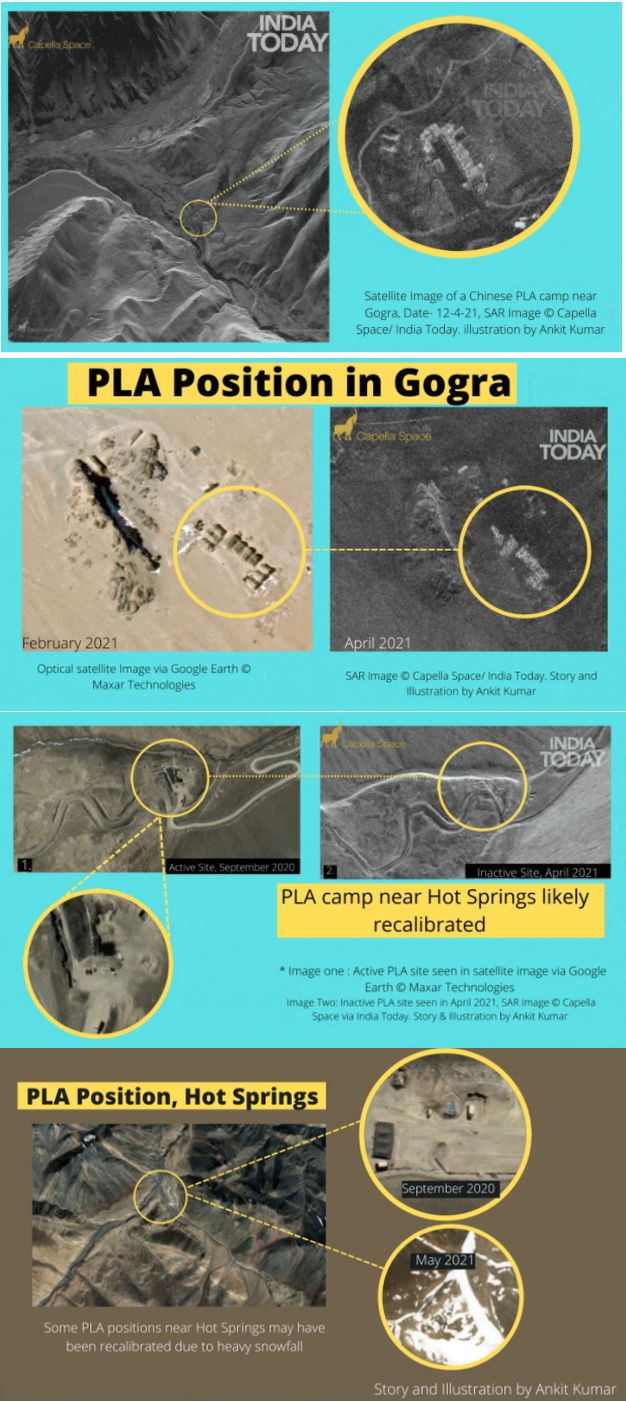
EXCLUSIVE: SATELLITE IMAGES CAPTURE CHINESE RECALIBRATIONS NEAR LADAKH
Mayanglambam Siromani, 32, was arrested for alleged involvement in an ambush on a road-opening party of 4th Assam Rifles in Manipur’s Chandel on 15 November 2017.
New Delhi: The NIA has arrested a self-styled lieutenant of the outlawed People’s Liberation Army/Revolutionary People’s Front for his alleged involvement in an ambush and killing of an Assam Rifles official in Manipur, an official said on Friday.
Mayanglambam Siromani, 32, of Manipur’s Kakching district was arrested by the premier investigation agency on Thursday. He had fled India and taken shelter in Myanmar after the ambush.
The case is related to an ambush on a road-opening party of 4th Assam Rifles at Chamol-Sajik Tampak Road in Manipur’s Chandel in 2017 in which one Assam Rifles official was killed and another injured. Two terrorists were also killed in the encounter.
Militants carried out the ambush on November 15, 2017 when a unit of the 4th battalion of the Assam Rifles was conducting a road opening task on the Chamol-Sajir Tampak road in Chandel district.
The NIA probe established that the militants conspired to wage war against the Government of India and in furtherance of this conspiracy, they ambushed the Assam Rifles team, the official said.
Siromani was involved in the conspiracy to attack the road opening party of Assam Rifles. Based on the evidence, he was chargesheeted while being on the run. Further, he was declared a proclaimed offender and a cash reward of Rs 2 lakh was announced for information leading to his apprehension, the official added.
He was an active operative of the PLA/RPF in the 252 mobile battalion of PLA/RPF based in Myanmar.
He along with his co-accused had escaped after the ambush to Myanmar. The accused was produced before a special NIA court in Imphal and taken on police remand for five days, the official said.
Further investigation into the case is underway, he added.
The demand for handing over control to the armed forces is primarily due to loss of confidence in existing infrastructure, besides inefficient logistics. Shortages have been exacerbated due to profiteering and cornering of resources. The armed forces can help in setting up centralised war rooms and coordinated communications network. The biggest gain would be the elimination of local manipulation.
UNDER STRAIN: Health infrastructure has been under pressure amid the pandemic. PTI
Lt Gen KJ Singh (retd)
Former GOC-in-C, Western Command
As the nation battles the mega second wave of Covid along with an infodemic tsunami, questions that rankle the hapless and desperate population are — when will the armed forces take over and why are they not being given responsibilities of oxygen supply and managing hotspots like Delhi? Two former Army commanders and many senior veterans have felt that the forces are being utilised sub-optimally. Yet, the government has stated in court that it cannot ask the Army to take over in Delhi. The Delhi High Court has concurred with this argument.
The forces have finite medical resources and the existing medical system in Delhi, even in normal times, works on support from the field hospitals of formations in the vicinity. Unlike civil hospitals, paramedical and nursing support in Military Hospitals (MHs) and Base Hospitals (BHs) has been a cause for concern. This can be attributed to spartan manning norms. The flexibility in the emergency response system was further eroded with the winding up of medical TA (Territorial Army) civil hospitals in 2014.
An objective assessment would establish that niche capabilities, especially in logistics of forces, including the Air Force and the Navy, are being extensively utilised. It is most evident in the transportation of cryogenic oxygen plants and containers. The Corps of Electronics and Mechanical Engineers (EME) has also repaired and resuscitated non-functional oxygen generation plants. In addition, the forces have helped to set up the Defence Research and Development Organisation (DRDO) hospitals, including manning them. It is a matter of concern that locations for the so-called DRDO hospitals appear to have been chosen more for optics and parochial considerations. Even the naming of such temporary facilities has some political overtones. It would be better to honour medics like Maj Laishram Singh (Ashok Chakra) and the Covid Yodhas by naming them
The MHs have raised bed capacities by 10-15% to accommodate civilian patients, subject to availability. It also bears mention that the veterans are up in arms and letters have been shot off to the Raksha Mantri (RM) lamenting this step, even when many veterans are running from pillar to post to find beds. This fact has been acknowledged and put on record by the MoD, which has questioned the very relevance of the Ex-servicemen Contributory Health Scheme (ECHS).
The unfortunate part is that bureaucrats prefer to raise objections and queries, whereas they are responsible for finding solutions. It is indeed time to fix accountability, release adequate funds and reduce the pendency of unpaid bills. The bottom line is that the liability of healthcare for veterans is absolutely non-negotiable. While it is accepted that the system is literally swamped, yet more empathy and better communication will help to alleviate the veterans’ plight to some extent.
The demand for handing over the situation to the armed forces is primarily due to loss of confidence in the existing crumbling infrastructure and inefficient logistics. Shortages have been exacerbated due to most reprehensible tendencies of profiteering and cornering of resources by the power brokers and fixers. The only solution is nabbing them and exemplary punishment through fast-track tribunals. Such criminals should be publicly shamed and socially ostracised. Contrived shortages have fuelled rumours and panic.
The armed forces can help in setting up centralised war rooms and coordinated communications network extending to regional nodes. Oxygen supplies and distribution can be managed by departmental TA units, which have domain competence in supply and distribution. These units can be assisted by a regular technical and logistics unit, which can handle any situation. The biggest gain would be the elimination of local manipulation.
The present government has junked a large number of colonial-era laws, but our response is still driven by the Epidemic Diseases Act, 1897. It is time a contemporary statute is drafted and operationalised. Concurrently, the Disaster Management Act, 2005, should be updated and include an addendum on pandemics and health emergencies. Notwithstanding the fact that ‘emergency’ is abhorred in political lexicon, yet it will be a good idea to lay down norms for national emergencies. With our resilience, we should be able to overcome this crisis, but it is axiomatic that we learn lessons and are better prepared to avert the next lurking challenge. The frequency of such emergencies in all probability is likely to increase in future.
The response has to be institutionalised and driven by statutory and mandated bodies. The NDMA and NDRF are not seen to be active, it will be appropriate that they are empowered in staffing and given due authority. Even states, except a few like Orissa, have notional state-level structures. Our disaster management matrix is based on response time and quantum of force. In all eventualities, the first responders have to be well-trained organic elements, civil defence, Home Guards and the police. In remote areas, the Army, due to its location, could also be concurrent, the first responder. They have to be supplemented with the NDRF, CAPFs, armed forces and NGOs, depending on the scale of tragedy.
The NDRF is the designated primary responder, but has very limited capacities and only nominal ones in public health. Secondary responders include all others with the Army called in only as the ultimate responder. The raising of the NDRF and proliferation of demand for the Army has resulted in marked hesitancy on the part of the forces to get sucked into routine functions. Capability building for disaster relief in the forces needs to be funded. It is worrying that the forces are not represented in any of the 11 empowered committees and even the Supreme Court has not included them in the specially constituted task force, despite a stellar record and domain competence. It is time the expertise of forces is tapped in planning and management of critical functions.
Armed forces rope in Battlefield Nursing Assistants to help in Covid care
The services are pitching in every field of national effort towards Covid-19 relief
90 personnel, including anaesthesiologists, physicians, medical officers, nursing staff and paramedical staff been flown from various Naval Stations to Ahmedabad for COVID-19 duties. — PTI
New Delhi, May 14
The armed forces have roped in Battlefield Nursing Assistants (BFNA) to help fight the second wave of COVID-19 and have suggested that a similar model can be followed by state governments and hospitals, according to senior officials.
Lt General Madhuri Kanitkar, the Deputy Chief of Integrated Defence Staff (Medical), believes BFNAs can also train young volunteers to help relieve trained nurses of administration duties so that they can be gainfully utilised for more important duties in the fight against the pandemic.
The armed forces are pulling out all available resources to augment its ‘Ops CO-JEET’, a joint effort of the Army, the Indian Air Force and the Navy against the pandemic, and have deployed BFNAs at COVID-19 care centres.
BFNAs are generally trained in providing basic health care facilities in combat situation which include administering injections and helping in breathing exercise, Lt Gen Kanitkar said.
The armed forces are even helping the state administrations by putting to use their personnel and military resources to provide succour to the needy, but more is required to be done in these testing times and, therefore, volunteers from the society are needed to assist the state governments, she said.
Lt Gen Kanitkar also said a large number of Battlefield Nursing Assistants who are trained in basic medical care have been brought in for COVID-19 management.
“We have created a mechanism where we are trying for a dedicated buddy for 25 patients,” the Lt General said.
Already the fresh COVID-19 wave has been treated as a war and the armed forces have launched the operation “CO-JEET” which encompasses psychological measures to allay fears and panic and augmentation of medical facilities to combat the disease.
Carrying on with the belief of ‘conviction theory’ that “in times of stress, if you have someone to talk to, it makes a huge difference”, Lt Gen Kanitkar said the nursing assistants from the Army, the IAF and the Navy would reassure COVID-19 patients that everything will be fine soon.
“In case of need, these soldiers who are already trained in providing basic nursing aid during combat operations would help in respiratory issues by making the patients do breathing exercise,” she said.
The “Co-JEET” operation has engaged the personnel of the three wings of the armed forces—the Army, Indian Air Force and the Navy—to help restore the oxygen supply chain, setting up of COVID-19 beds and providing help to civilian administration in their fight to control the pandemic.
The Department of Defence created a Covid crisis Management Committee. The CO-JEET stands for Co-workers of all the three services who will finally have ‘Jeet’ (victory) over Covid.
Having vaccinated close to 98 per cent of the workforce, the services are pitching in every field of national effort towards COVID-19 relief while maintaining seamless coordination with government machinery to ensure optimisation of medical efforts.https://9da6deb2580e1f386badc826bd09a3c1.safeframe.googlesyndication.com/safeframe/1-0-38/html/container.html
This move is part of the concerted efforts to upgrade the facilities of armed forces’ hospitals which are being run beyond their capacity by the depleted medical manpower, she added
Online medical consultation service by retired military doctors rolled out for entire country
A COVID-19 patient on oxygen support waits to be admitted at Patna Medical College and Hospital, during the second wave of coronavirus in Patna on Friday. PTI photo
New Delhi, May 14
A free online medical consultation service launched by retired military doctors in view of a massive surge in coronavirus cases in India was on Friday extended to citizens across the country, officials said.
The defence ministry roped in retired military doctors to provide online consultations to civilian patients under a telemedicine platform.
The service was rolled out on May 7 for Uttar Pradesh and extended to Rajasthan and Uttarakhand days later as more veteran defence volunteer doctors came on board.
Currently, 85 veteran defence doctors are providing their services on the portal and have provided online consultation to more than 1,000 patients, according to the defence ministry.
“After the successful roll out in three states, ex-defence OPD, now renamed as Defence National OPD, has been rolled out pan-India on May 14 and is available on www.esanjeevaniopd.in,” it said in a statement.
It said the vast experience of the military doctors is being optimally utilised.
“This initiative will go a long way in obtaining necessary medical advice and consultation in the safe environment of patients’ homes, avoiding unnecessary visits to hospitals and increasing the risk of getting infected with COVID and overburdening the limited health resources,” the ministry said.
The service was launched under the e-Sanjeevani OPD platform of the Union health ministry.
The e-Sanjeevani OPD is a flagship telemedicine platform of the government developed by the Centre for Development of Advanced Computing (C-DAC). — PTI
State Stalwarts
DEFENCE MINISTER
Minister Rajnath Singh
ALL HUMANS ARE ONE CREATED BY GOD
HINDUS,MUSLIMS,SIKHS.ISAI SAB HAI BHAI BHAI
CHIEF PATRON ALL INDIA SANJHA MORCHA
LT GEN JASBIR SINGH DHALIWAL, DOGRA
SENIOR PATRON ALL INDIA SANJHA MORCHA
MAJOR GEN HARVIJAY SINGH, SENA MEDAL ,corps of signals
.
.
PATRON ALL INDIA SANJHA MORCHA
MAJ GEN RAMINDER GURAYA ,MADRAS REGIMENT
sanjhamorcha303@gmail.com
PRESIDENT SOUTH ALL INDIA SANJHA MORCHA
COL SS RAJAN BOMBAY SAPPERS,
PRESIDENT UTTARAKHAND ALL INDIA SANJHA MORCHA
COL B M THAPA ,BENGAL SAPPERSS
PRESIDENT HARAYANA STATE CUM COORDINATOR ESM
BRIG DALJIT THUKRAL ,BENGAL SAPPERS
PRESIDENT TRICITY
COL B S BRAR (BHUPI BRAR)
PRESIDENT CHANDIGARH ZONE
COL SHANJIT SINGH BHULLAR
.
.
PRESIDENT PANCHKULA ZONE AND ZIRAKPUR
COL SWARAN SINGH
INDIAN DEFENCE FORCES
DEFENCE FORCES INTEGRATED LOGO
INDIAN AIR FORCE
Air Officer C-in-C WESTERN AIR COMMAND
AIR MSHL S PRABHAKARAN AVSM VM
AOC-IN-C, EASTERN AIR COMMAND
Air Marshal Inderpal Singh Walia
AOC-in-C SOUTH WESTERN AIR COMMAND
Air Marshal Vikram Singh
AOC-IN-C, SOUTHERN AIR COMMAND
Air Marshal J.Chalapati
AOC-IN-C TRAINING COMMAND
AIR MARSHAL SK GHOTIA VSM
AOC-IN-C MAINTENANCE COMMAND
Air Marshal Jagdish Chandra
Flag Officer Commanding in Chief, Western Naval Command
ice Admiral R Hari Kumar, PVSM, AVSM, VSM
Flag Officer Commanding in Chief, Eastern Naval Command
Vice Admiral Sanjay Bhalla, AVSM, NM
Flag Officer Commanding in Chief, Southern Naval Command